


Plasmapheresis and Autoimmune Disease: What Patients Should Know
Living with an autoimmune disease means your immune system has turned against your own body, producing antibodies that attack healthy tissues instead of protecting them. For many patients, finding effective treatment can feel like an ongoing challenge. Plasmapheresis autoimmune disease treatment offers a powerful option that directly removes these harmful antibodies from your blood, providing relief when other treatments fall short.
This comprehensive guide explains how plasmapheresis autoimmune disease treatment works, which diseases respond best, what the research shows about effectiveness, and what you can expect if your doctor recommends this therapy for your autoimmune disorder. Whether you've just been diagnosed or you're exploring treatment options after other therapies haven't worked, this evidence-based information will help you understand your choices.
[banner2]
How Plasmapheresis Works for Autoimmune Disease
Plasmapheresis, also called therapeutic plasma exchange (TPE), is a medical procedure that filters your blood to remove harmful substances from the plasma—the liquid portion that carries antibodies, proteins, and other components. Understanding how plasmapheresis autoimmune disease treatment works starts with understanding what goes wrong in autoimmune conditions.
In autoimmune diseases, your immune system produces autoantibodies—antibodies that mistakenly target your own tissues. In myasthenia gravis, these antibodies attack the connections between nerves and muscles. In lupus, they can target multiple organs. In neuromyelitis optica, they attack specific proteins in the nervous system. These circulating autoantibodies cause ongoing damage as long as they remain in your blood.
Plasmapheresis for autoimmune disease works by physically removing these harmful antibodies. During the procedure, blood is drawn from your body, separated into plasma and blood cells using a specialized machine, and then the plasma containing the damaging antibodies is discarded. Your blood cells are returned to you along with a replacement fluid—typically albumin solution—creating fresh plasma without the disease-causing antibodies.
This approach differs fundamentally from medications that suppress immune function. While immunosuppressants slow down antibody production, plasmapheresis autoimmune treatment removes antibodies that already exist. A single session can reduce antibody levels by 60-80%, providing rapid relief that medications alone cannot achieve (International Journal of Molecular Sciences, 2018).
The speed of plasmapheresis makes it particularly valuable for autoimmune crises. When a patient experiences a severe flare or life-threatening symptoms, waiting weeks for medications to take effect isn't always an option. Plasmapheresis and autoimmune disease management often work together—the procedure provides immediate antibody reduction while longer-term immunotherapy prevents new antibody formation.
Autoimmune Conditions Treated with Plasmapheresis
Plasmapheresis autoimmune disorders treatment has been studied extensively across many conditions. The American Society for Apheresis (ASFA) publishes guidelines categorizing treatments by evidence strength: Category I indicates first-line therapy, Category II means second-line or adjunctive therapy, Category III requires individual assessment, and Category IV indicates the treatment is ineffective or harmful (Connelly-Smith et al., 2023).
Here's what you should know about plasmapheresis for specific autoimmune conditions:
Myasthenia Gravis
Myasthenia gravis (MG) causes muscle weakness when autoantibodies block communication between nerves and muscles. Plasmapheresis autoimmune disease treatment for MG has some of the strongest evidence of any application.
Research shows response rates between 57% and 100% for plasmapheresis in myasthenia gravis, with a meta-analysis demonstrating that TPE achieves a 19% higher response rate compared to intravenous immunoglobulin (IVIG) in acute MG crises (Benatar et al., 2021). Plasmapheresis is particularly valuable for:
Myasthenic crisis (severe weakness affecting breathing)
- Preparation before thymectomy surgery
- Rapid stabilization when symptoms worsen suddenly
- Cases not responding adequately to medications
Most patients notice improvement within days of starting treatment, with maximum benefit typically achieved within 4-6 weeks.
Neuromyelitis Optica Spectrum Disorder (NMOSD)
NMOSD causes inflammation in the optic nerves and spinal cord, leading to vision problems and paralysis. The culprit is usually an autoantibody targeting a protein called aquaporin-4. Plasmapheresis autoimmune disease treatment for NMOSD directly removes these anti-AQP4 antibodies.
Studies show that plasmapheresis reduces anti-AQP4 antibody levels to just 15% of pre-treatment levels, with 50% of patients showing significant improvement immediately after treatment and 78% improved at six-month follow-up (Journal of Neurology, 2013). The treatment works best when started early in an acute attack and combined with high-dose corticosteroids.
Autoimmune Encephalitis
Autoimmune encephalitis occurs when antibodies attack the brain, causing confusion, seizures, psychiatric symptoms, and movement disorders. Various antibody types can cause this condition, including anti-NMDA receptor, anti-LGI1, and anti-GABAb antibodies.
Plasmapheresis and autoimmune disease of the brain shows impressive results. Research demonstrates that 64% of patients improve within one month of plasmapheresis treatment, increasing to 94% at two months—compared to just 33% and 67% respectively without plasmapheresis (Zhang et al., 2021). The procedure is especially valuable as rescue therapy when steroids and IVIG don't provide adequate improvement.
Systemic Lupus Erythematosus (Lupus)
Lupus can affect virtually any organ system, with autoantibodies targeting DNA, cell membranes, and various proteins throughout the body. Plasmapheresis autoimmune disorders treatment for lupus is typically reserved for severe manifestations, including:
Lupus nephritis (kidney involvement) not responding to standard therapy
- Catastrophic antiphospholipid syndrome
- Severe lupus flares with organ-threatening complications
- Thrombotic thrombocytopenic purpura associated with lupus
While not a first-line treatment for routine lupus management, plasmapheresis can be life-saving in severe cases by rapidly removing the antibodies and immune complexes driving organ damage.
ANCA-Associated Vasculitis
These conditions—including granulomatosis with polyangiitis and microscopic polyangiitis—involve antibodies (ANCA) that cause blood vessel inflammation, potentially damaging kidneys, lungs, and other organs.
The evidence for plasmapheresis autoimmune disease treatment in ANCA vasculitis is nuanced. The MEPEX trial showed improved kidney recovery (69% vs 49%) with plasmapheresis in severe cases, though the larger PEXIVAS trial found less dramatic overall differences (Journal of Clinical Medicine, 2021). Current guidelines recommend plasmapheresis for:
Severe kidney involvement (creatinine >5.7 mg/dL)
- Patients requiring dialysis
- Diffuse alveolar hemorrhage (bleeding into the lungs)
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
CIDP causes progressive weakness and sensory changes due to immune attack on peripheral nerve coverings. Plasmapheresis autoimmune disease treatment shows response rates of 33-66% in CIDP patients, making it an established second-line option when other treatments provide insufficient benefit.
Multiple Sclerosis
For multiple sclerosis, plasmapheresis is primarily used for severe relapses that don't respond to high-dose corticosteroids. Response rates reach approximately 80% in relapsing-remitting MS, though the treatment is less effective for progressive forms of the disease. Plasmapheresis and autoimmune disease management in MS focuses on acute rescue rather than long-term maintenance.
Other Conditions
Plasmapheresis autoimmune disease applications extend to several other conditions, including:
Guillain-Barré Syndrome (ASFA Category I)
- Autoimmune hemolytic anemia
- Inflammatory myopathies (dermatomyositis, polymyositis)
- Pemphigus and pemphigoid (severe autoimmune skin conditions)
What the Research Shows: Efficacy and Evidence
Understanding the evidence behind plasmapheresis autoimmune disease treatment helps you have informed conversations with your healthcare team. Here's what decades of research tell us:
ASFA Guidelines Explained
The American Society for Apheresis evaluates treatments based on available evidence and assigns categories:
Category I: First-line treatment, either alone or with other therapies
- Category II: Second-line treatment, either alone or with other therapies
- Category III: Optimal role not established; individual decision required
- Category IV: Published evidence shows treatment is ineffective or harmful
Most autoimmune applications fall into Category I or II, indicating solid evidence supporting use. The 2023 guidelines include 166 indications across 91 conditions, with autoimmune diseases representing a significant portion (Connelly-Smith et al., 2023).
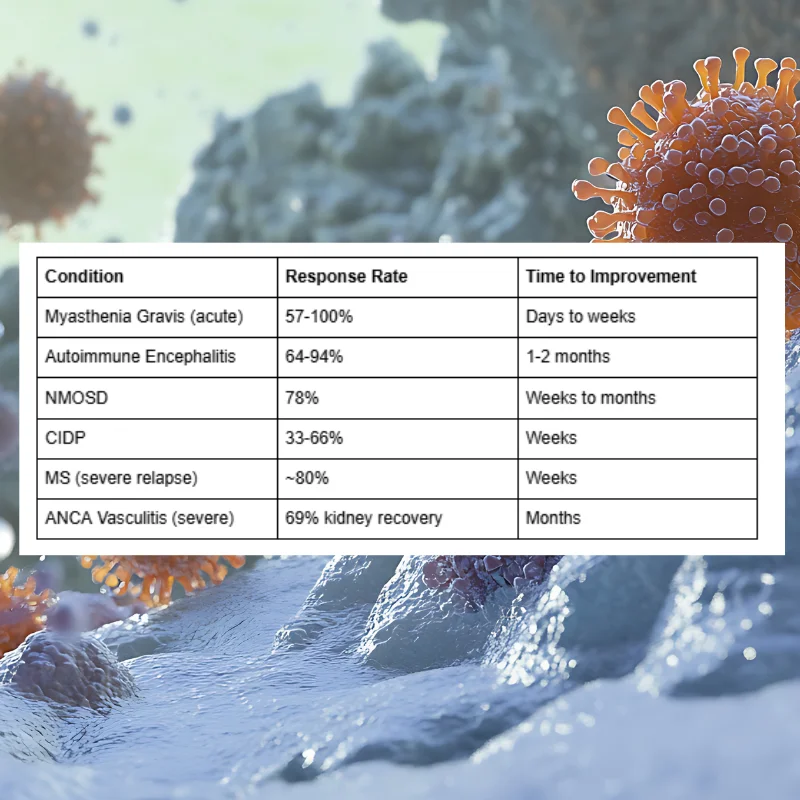
Response Rate Summary
Based on published research, here's what patients can expect from plasmapheresis autoimmune disorders treatment:
What "Response" Means Practically
When research reports a "response rate," it typically means measurable clinical improvement—reduced weakness scores, improved function, or stabilization of disease progression. For patients, this often translates to:
Ability to perform daily activities that were previously difficult
- Reduced medication requirements
- Shorter hospital stays
- Prevention of irreversible damage during acute flares
- Improved quality of life scores
A study on myasthenia gravis found that patients receiving plasmapheresis achieved functional improvement within 4 weeks 57% of the time, compared to 35% without the treatment, and required mechanical ventilation less often (14% vs 27%) (Egyptian Journal of Neurology, Psychiatry and Neurosurgery, 2021).
Plasmapheresis vs Other Autoimmune Treatments
Understanding how plasmapheresis autoimmune disease treatment compares to alternatives helps you understand where it fits in your care plan.
Plasmapheresis vs IVIG
Intravenous immunoglobulin (IVIG) is another common treatment for autoimmune conditions. Both remove or neutralize harmful antibodies, but they work differently:
Plasmapheresis advantages:
Faster onset of action
- Directly removes existing antibodies
- Higher response rate in some conditions (+19% in acute MG)
- May work when IVIG hasn't helped
IVIG advantages:
Easier administration (doesn't require specialized equipment)
- Can be given in outpatient settings
- No need for large-bore IV access
- Fewer immediate side effects for some patients
Research suggests plasmapheresis autoimmune disease treatment provides faster improvement, with one study showing maximum benefit at 6.5 weeks versus 7.1 weeks for IVIG. Your doctor may recommend one over the other based on your specific condition, symptom severity, and practical considerations.
Plasmapheresis vs Immunosuppressants
Immunosuppressive medications (like azathioprine, mycophenolate, or rituximab) work by reducing immune system activity and slowing antibody production. Plasmapheresis and autoimmune disease medications often work together:
Plasmapheresis removes existing antibodies quickly
- Immunosuppressants prevent new antibody formation over time
- Combination therapy addresses both immediate and long-term needs
This complementary approach is particularly common in conditions like myasthenia gravis and NMOSD, where rapid symptom control and sustained remission are both important goals.
Emerging Alternatives
Newer treatments like FcRn inhibitors (efgartigimod, rozanolixizumab) offer another way to reduce harmful antibodies. These medications block the recycling of IgG antibodies, causing them to break down faster. While promising, they don't provide the immediate, dramatic antibody reduction that plasmapheresis autoimmune disorders treatment achieves, making plasmapheresis still essential for acute crises.
What to Expect During Plasmapheresis for Autoimmune Disease
Knowing what happens during treatment helps reduce anxiety and allows you to prepare appropriately.
Before Treatment
Your medical team will:
Review your medical history and current medications
- Check blood tests (complete blood count, clotting factors, electrolytes)
- Establish vascular access (peripheral IV or central line, depending on your veins and treatment duration)
- Explain the procedure and answer your questions
During Each Session
A typical plasmapheresis autoimmune disease treatment session involves:
Duration: 2-4 hours per session
- Position: Lying or reclining comfortably
- Process: Blood flows through a machine that separates plasma from blood cells
- Replacement: Your blood cells return with albumin solution replacing the removed plasma
- Monitoring: Staff check vital signs and watch for any reactions throughout
Many patients read, watch videos, or rest during treatment. Some experience mild symptoms like tingling around the mouth or fingertips (from citrate, an anticoagulant used during the procedure), which staff can address with calcium supplements.
Treatment Course
For most plasmapheresis autoimmune disease conditions, a typical course includes:
Number of sessions: 3-7 treatments (sometimes more for severe cases)
- Frequency: Every other day or 3 times per week
- Total duration: 1-3 weeks for a treatment course
- Repeat courses: May be needed for flares or as maintenance in some conditions
Timeline for Improvement
How quickly you'll notice improvement depends on your specific condition:
Myasthenia gravis: Often within days; maximum improvement in 4-6 weeks
- Autoimmune encephalitis: Gradual improvement over 1-2 months
- NMOSD: Immediate improvement in 50%; continued improvement over months
- Severe relapses: Stabilization within days, recovery over weeks
Safety, Side Effects, and Risks
Like any medical procedure, plasmapheresis carries potential risks. Understanding these helps you recognize problems early and feel confident about treatment.
Common Side Effects
Most side effects from plasmapheresis autoimmune disease treatment are mild and manageable:
Citrate reactions (most common):
- Tingling around mouth, fingers, or toes
- Muscle cramps
- Caused by the anticoagulant binding calcium temporarily
- Treated easily with oral or IV calcium
Hypotension (low blood pressure):
Occurs in about 8% of procedures
- Usually mild, causes lightheadedness
- Managed by adjusting fluid replacement and slowing the procedure
Fatigue:
Common after sessions
- Usually resolves within a day
- Plan for rest on treatment days
Less Common Risks
More significant complications occur in a minority of patients:
Infection risks:
Higher with central venous catheters than peripheral IVs
- Prevented through sterile technique and proper catheter care
- Signs to report: fever, redness, or drainage at catheter site
Allergic reactions:
More common if fresh frozen plasma (FFP) is used instead of albumin
- May include hives, fever, or rarely more severe reactions
- Staff are trained to recognize and treat these promptly
Bleeding or clotting:
Removal of clotting factors can temporarily increase bleeding risk
- Central lines carry small risk of blood clots
- Minimized through monitoring and appropriate anticoagulation
Risk Factors and Safety Data
Research shows the overall serious adverse event rate is approximately 5-15% of patients, with most complications being manageable (Medicina, 2023). Risk is influenced by:
Access type: Peripheral IV access has fewer complications than central lines
- Patient factors: Overall health, age, and specific condition
- Experience of treatment center: Higher-volume centers typically have better outcomes
Your medical team will discuss your individual risk factors and take steps to minimize complications. The benefits of plasmapheresis autoimmune disease treatment typically outweigh risks for appropriate candidates, which is why it remains a recommended therapy in major guidelines.
Is Plasmapheresis Right for Your Autoimmune Condition?
Determining whether plasmapheresis autoimmune disorders treatment is appropriate for you involves several considerations.
When Plasmapheresis Is Typically Recommended
Your doctor may recommend plasmapheresis and autoimmune disease treatment if you:
Are experiencing an acute crisis or severe flare
- Haven't responded adequately to first-line treatments
- Need rapid stabilization before surgery
- Have severe organ involvement requiring immediate intervention
- Have a condition with strong evidence supporting plasmapheresis use
Questions to Ask Your Doctor
Before starting treatment, consider asking:
"Is my specific condition appropriate for plasmapheresis?" - Not all autoimmune diseases respond equally well
- "What response rate can I realistically expect?" - Understanding likely outcomes helps set expectations
- "How many sessions will I need, and how often?" - Helps with practical planning
- "What are my alternatives if I don't do plasmapheresis?" - Understanding options supports informed decisions
- "What side effects should I watch for?" - Knowing what's normal vs concerning
- "Will I need repeat treatments in the future?" - Some conditions require periodic maintenance
- "How will plasmapheresis fit with my other treatments?" - Understanding the overall care plan
Finding the Right Treatment Center
Plasmapheresis autoimmune disease treatment should be performed by experienced teams with:
Specialized apheresis equipment and trained staff
- Physicians experienced in your specific condition
- Ability to manage potential complications
- Coordination with your other healthcare providers
Conclusion
Plasmapheresis and autoimmune disease treatment represents one of the most direct approaches available for conditions driven by harmful autoantibodies. By physically removing these disease-causing antibodies, plasmapheresis autoimmune disease treatment provides rapid relief that can be life-changing—and sometimes life-saving—for patients in crisis or those who haven't found adequate relief from other therapies.
The evidence supporting plasmapheresis autoimmune disorders treatment is substantial, with decades of research and clear guidelines from organizations like ASFA. Response rates of 57-100% for myasthenia gravis, 64-94% for autoimmune encephalitis, and strong results across many other conditions demonstrate that this isn't experimental therapy—it's established medicine with proven benefits.
If you're living with an autoimmune condition and wondering whether plasmapheresis might help, the information in this guide provides a foundation for discussing options with your healthcare team. Every patient's situation is unique, and the decision involves weighing your specific condition, symptom severity, response to other treatments, and personal circumstances.
At Humanaut Health, we offer therapeutic plasma exchange as part of our comprehensive approach to advanced medical care. Our experienced team understands the nuances of plasmapheresis autoimmune disease treatment and works closely with patients to deliver personalized care. If you'd like to learn more about whether plasmapheresis might be appropriate for your condition, we welcome the opportunity to discuss your options.
References


